Table of Contents
- Hormones and Migraines
- Migraines and Hormones: How Hormones Affect Migraine Sensitivity
- Key Hormones Influencing Migraine Sensitivity
- Life Stages and Hormonal Patterns
- Hormone Replacement Therapy and Migraines
- Non-Hormonal Factors that Interact with Hormones
- Practical Strategies for More Stable Days
- See also:
- Brain Ritual® Support
- FAQs
- What do people mean by “hormonal migraines”?
- What causes migraines in females?
- Is migraine in men related to hormonal change, or a different mechanism?
- Can hormones cause migraines?
- Are bioidentical hormones preferable for people with migraine?
- What helps hormonal migraines feel more manageable?
- How is estrogen withdrawal different from other hormonal fluctuations in migraine?
- Do hormones other than estrogen and progesterone play a role in migraine?
- Can hormonal contraception, such as the contraceptive pill, affect migraine patterns?
- Why do hormonal migraine patterns change over time?
- Final Thoughts
- References
At a Glance
|
Hormones and Migraines
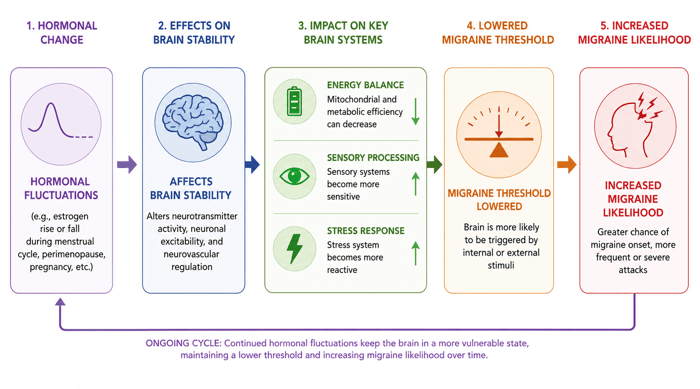
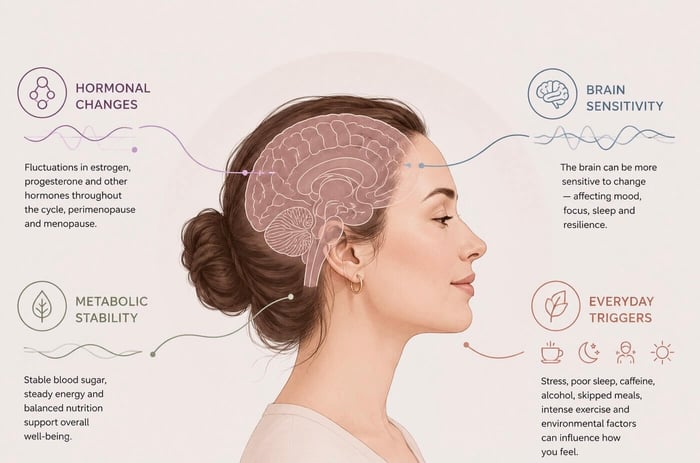
Hormones play a meaningful role in how your body regulates energy, sleep, stress, inflammation, and sensory processing. These same systems are closely linked to migraine sensitivity, which is why you may feel more susceptible to migraine when hormones shift during the month or at major life-stage changes.
Many women notice shifts in migraine sensitivity around the menstrual cycle, during early pregnancy, or in the weeks after giving birth; this is sometimes referred to as a hormonal migraine. These patterns can change again in perimenopause and menopause, or when stress or disrupted sleep adds pressure to the system. Smaller day-to-day fluctuations in hormone activity can also influence how reactive the brain feels. Migraine affects men as well, and while their hormone fluctuations follow steadier patterns, shifts in stress, sleep, and daily routine can still affect their sensitivity.
Understanding how hormones affect the biological systems that contribute to migraine sensitivity can make it easier to notice when a bit of added support or steadier habits may be helpful. Let’s take a closer look at how hormonal shifts interact with energy metabolism, inflammation, sensory processing, and sleep.
Migraines and Hormones: How Hormones Affect Migraine Sensitivity
Hormones are chemical messengers released by glands and carried through the bloodstream to different parts of the body. They help coordinate how key systems function and respond to change.
Hormones influence several core biological systems that are involved in migraine sensitivity. These systems involve energy metabolism, inflammatory and immune signaling, sensory processing, and the regulation of sleep and circadian rhythms. When hormone levels fluctuate, the stability of the body’s regulatory pathways can change, which may affect how easily the brain reaches its migraine threshold. The following sections outline how these pathways work and why hormonal fluctuations can make some people more responsive to internal and external triggers.
Energy and Metabolic Signaling
Hormones help regulate how the brain produces and uses energy. Estrogen, cortisol, insulin, and thyroid hormones each play roles in mitochondrial function, glucose regulation, and metabolic stability. When hormone levels fluctuate, it can become more difficult to maintain steady energy levels, leading to greater sensitivity to changes in routine or demand.
Estrogen helps support mitochondrial efficiency and influences how neurons use glucose for energy.
Cortisol affects energy availability during stress and can influence blood sugar levels.
Insulin plays a central role in glucose regulation, and fluctuations may contribute to energy dips or spikes that can influence migraine sensitivity.
Thyroid hormones, particularly triiodothyronine (T3) and thyroxine (T4), help regulate metabolic rate and temperature, both of which shape overall energy stability.
Disrupted eating patterns, low blood sugar, or increased metabolic demand may coincide with hormonal fluctuations.
Nutrients involved in cellular energy, such as CoQ10 and magnesium, help support the metabolic pathways involved in energy regulation.
Did you know?
Hormonal fluctuations can shift neuronal energy requirements faster than mitochondrial and glucose-regulating pathways can adapt. This imbalance may lower the threshold for migraine symptoms, especially when combined with metabolic stress or inconsistent eating.
See also: metabolic migraine, CoQ10 migraine, migraine vs tension headache.
Inflammation and Immune Signaling
Hormonal fluctuations affect how the body regulates inflammatory and immune pathways. Estrogen, progesterone, and cortisol can all interact with mediators involved in these responses, which may affect how sensitive the brain feels during certain phases of the cycle or times of stress. These same shifts can also influence oxidative stress; a process closely tied to inflammatory balance.
Immune signaling and inflammatory activity influence pain pathways, circulation, and the brain’s ability to maintain internal stability. Hormonal fluctuations may alter how well these processes are regulated, particularly when additional triggers are present.
Estrogen helps modulate inflammatory mediators involved in vascular, pain, and immune responses.
Variations in progesterone levels modulate immune pathways and influence patterns of inflammatory regulation.
Cortisol helps regulate inflammation during times of stress. When cortisol rhythms become disrupted, inflammatory responses may be harder to manage.
Histamine and other immune-related mediators may fluctuate in activity around hormonal changes, particularly during the menstrual cycle.
Pre-existing inflammatory or immune-related conditions may become more apparent when hormone levels fluctuate, especially when oxidative stress is elevated.
Did you know?
Shifts in estrogen and cortisol can influence how immune cells release inflammatory mediators. Rapid changes in either hormone may make these pathways more reactive, especially when other triggers are present. This heightened reactivity can also influence vascular tone and neuroimmune signaling, both of which are involved in the early stages of migraine activation.
See also: migraine oxidative stress, migraine and sinus headache, histamine and migraines, can mold cause migraines, Lyme and migraines.
Sensory Processing and Pain Modulation
Hormonal fluctuations can influence how the brain processes sensory information, such as sensitivity to light, sound, movement, and environmental changes. These shifts may change how strongly the brain filters or amplifies sensory signals. This can make the brain feel more reactive during certain cycle phases or periods of stress.
Sensory pathways interact closely with pain-modulating networks in the brainstem and cortex. When hormone levels fluctuate, these systems may become more sensitive or less steady, especially if multiple triggers overlap.
Estrogen influences neurotransmitter systems involved in sensory filtering, such as serotonin pathways that help regulate visual and sound sensitivity.
Progesterone influences pain-modulating pathways in the brain, which can affect how strongly sensory input is perceived.
Fluctuations in cortisol during stress can heighten sensory alertness and increase the reactivity of pain-processing circuits.
Rapid hormonal changes can increase the excitability of sensory pathways, reducing the brain’s tolerance for light, motion, or visual contrast.
Sensory-related symptoms such as aura, altered pupil dilation, or brain fog may feel more noticeable during phases of hormonal instability.
Did you know?
Estrogen interacts with serotonin pathways involved in filtering and organizing sensory input. When estrogen levels rise or fall quickly, these pathways may become more reactive, increasing sensitivity to visual and auditory signals during shifting hormonal phases.
See also: aura migraine without headache, migraine brain fog, migraine pupil dilation, headaches and migraines, cluster Headache vs migraine.
Circadian Rhythm and Sleep Regulation
Circadian rhythms are internal biological cycles that regulate sleep, energy, hormone release, and how alert or restful you feel throughout the day. When these rhythms become disrupted, the brain finds it difficult to keep sensory processing smooth and energy use efficient.
Melatonin, cortisol, and the body’s sleep-wake patterns all interact to shape and maintain internal rhythms. Changes in hormone levels or daily routine can alter this balance and influence how sensitive the brain feels throughout the day.
Melatonin signals to the brain that it is time to rest. Changes in melatonin production influence how restorative sleep feels.
Cortisol follows a daily rhythm that supports morning alertness. When this rhythm becomes irregular, energy regulation and stress responses can become unsettled.
Hormonal fluctuations can shift sleep architecture, including changes in the depth and timing of different sleep stages.
Irregular light exposure, including evening screen use, blue-light input, or disrupted daylight patterns such as those from shift work, can interfere with melatonin release and sleep quality.
Poor or fragmented sleep can heighten next-day trigger sensitivity, especially during times of hormonal change.
Did you know?
The daily interplay between melatonin and cortisol helps regulate the internal circadian clock. When this cycle becomes misaligned because of disrupted sleep timing, stress, or hormonal fluctuations, the systems that control sensory and pain processing may shift in their responsiveness. This can contribute to differences in migraine sensitivity across the day.
See also: best way to sleep with migraine, red light therapy for migraines, can cold weather cause migraines, worst jobs for migraine sufferers.
Key Hormones Influencing Migraine Sensitivity
If hormone levels change more quickly than usual, the brain may become more reactive to internal or external triggers. The following sections outline the roles of key hormones and how their natural fluctuations may shape migraine patterns across different phases of life.
Estrogen
Estrogen plays a central role in how the brain regulates energy, sensory processing, inflammatory balance, and key neurotransmitter pathways. Fluctuations in estrogen levels, especially the dips that occur before menstruation or during perimenopause, can influence how sensitive the brain feels to triggers and how predictable migraine patterns become.
Estrogen helps stabilize several brain systems. Even normal cycle-related shifts can affect how predictable your migraine patterns feel.
As estrogen becomes more variable during perimenopause, migraine frequency or intensity may change.
Rapid changes in estrogen during early pregnancy and after childbirth can shift migraine patterns, especially when levels fall sharply postpartum.
Estrogen interacts with serotonin pathways involved in sensory filtering (the system that helps the brain process incoming sensory signals), which can influence sensitivity to light, sound, and visual patterns.
Low or rapidly changing estrogen levels may make aura symptoms more likely in people who already experience them.
Lifestyle factors such as stress, disrupted sleep, or irregular eating can intensify the effects of estrogen fluctuations.
Did you know?
Estrogen helps modulate serotonin signaling, a key pathway in sensory regulation and pain processing. When estrogen levels fluctuate quickly, this system can become less stable, which may help explain why visual sensitivity and aura symptoms become more noticeable during hormone-related life stages.
See also: are migraines a menopause symptom, estrogen and migraines with aura.
Progesterone
Progesterone is a hormone that helps regulate the menstrual cycle and supports early pregnancy. It also influences brain activity linked to mood, calmness, and pain modulation, which is why changes in progesterone levels can shape migraine patterns for some people.
Progesterone rises in the luteal phase and has a generally calming effect on neural activity. For some people, this can make sensory input feel less intense.
When progesterone levels drop before menstruation, the combined dip in progesterone and estrogen can influence how migraine patterns change.
By acting on pain-modulating networks, progesterone can alter how reactive the brain is to sensory input across cycle phases.
Sensitivity to progesterone-related changes varies between individuals. Some people notice mood or sleep shifts that indirectly affect migraine vulnerability.
Life stages such as early pregnancy and perimenopause influence progesterone patterns, which can in turn affect migraine predictability.
Did you know?
Progesterone interacts with GABA receptors, which inhibit excessive neural activity and support steadier brain signaling. When progesterone levels fluctuate, this inhibitory system can lose stability and influence the brain’s response to migraine triggers.
Cortisol
Cortisol supports the body’s ability to respond to stress and maintain circadian alertness, while also influencing immune balance and metabolic stability. Its levels naturally peak in the morning and fall gradually throughout the day. If this rhythm becomes irregular or cortisol rises more sharply in response to stress, the brain may become more reactive to migraine triggers.
Cortisol follows a daily rhythm, rising in the morning to support alertness and falling in the evening to prepare the body for rest.
Sudden rises in cortisol during stress can heighten sensory reactivity and lower migraine trigger thresholds.
Chronic stress or disrupted sleep can flatten normal cortisol rhythms, contributing to less predictable migraine patterns.
Cortisol helps regulate blood sugar, and fluctuations in its levels can influence energy stability in ways that make hormonal sensitivity feel stronger.
Life stages or conditions that alter cortisol levels, such as pregnancy, perimenopause, or adrenal disorders, may influence migraine frequency or severity.
Did you know?
Cortisol interacts closely with brain regions involved in regulating stress and sensory processing, including the amygdala, hippocampus, and prefrontal cortex. Rapid increases in cortisol can heighten the reactivity of these networks, partly explaining why stress-related triggers such as sensory overload or disrupted routines may lead to migraine in some people.
See also: migraine stress management.
Adrenaline
Adrenaline is released during moments of stress, excitement, or sudden shifts in the environment, and produces fast-acting changes throughout the body. It increases heart rate, boosts blood flow to muscles, heightens alertness, and sharpens the body’s readiness for rapid action. For people with migraine, sudden spikes in adrenaline can influence sensory sensitivity, tension patterns, and how easily the brain crosses the threshold for migraine symptoms.
Adrenaline triggers the “fight-or-flight” response, increasing alertness, heart rate, and muscle tension, all of which influence migraine sensitivity.
Sudden surges in adrenaline, such as during stress, strong emotions, or abrupt physical exertion, may lower the brain’s threshold for migraine activation.
Following stress, declining adrenaline levels may trigger symptoms in some people, especially if blood sugar or cortisol levels shift at the same time.
Adrenaline interacts with pain-modulating and sensory pathways, which can influence light and sound sensitivity, as well as neck and shoulder tension.
People who experience anxiety-related symptoms (e.g., racing heart, hypervigilance, shallow breathing) may find that adrenaline surges coincide with periods of increased migraine vulnerability.
Did you know?
Adrenaline acts strongly on the locus coeruleus, a brainstem region involved in arousal, sensory gain, and early pain modulation, and also affects wider networks involved in alertness and stress response. When adrenaline surges rapidly, this activity can amplify sensory input and increase neuronal excitability, which may help explain why emotional stress or sudden shock can trigger migraines in some people.
See also: why does my neck hurt when I have a migraine, understanding migraine triggers.
Melatonin
Melatonin helps regulate sleep timing, circadian alignment, nighttime recovery, and some of the cellular repair processes that take place during sleep. Its release increases in the evening as light intensity falls, helping the brain shift toward rest. When melatonin production is delayed, reduced, or disrupted, the transition into restorative sleep can become harder, which may influence next-day migraine sensitivity.
Melatonin helps signal when it is time to sleep, and reduced evening release can make it harder to achieve deep or continuous rest.
Melatonin acts as an antioxidant within mitochondria. When sleep is disrupted, this protective effect may be reduced, particularly during periods of higher oxidative load.
Irregular sleep, late-night screen exposure, or inconsistent light–dark cues can shift melatonin production and delay its usual rise before sleep.
Hormonal changes, especially shifts in cortisol or estrogen, can influence how consistently melatonin is produced.
Reduced melatonin levels or a delayed onset of its release can make the brain more sensitive to light, noise, or stress the next day.
People who experience insomnia, broken sleep, or irregular sleep-wake cycles often notice migraine patterns that align with these changes.
Did you know?
Although melatonin is produced in the pineal gland, its release is regulated by the suprachiasmatic nucleus, which serves as the brain’s central circadian clock. Melatonin plays an important role in mitochondrial antioxidant defence, which may help explain why disrupted sleep can feel especially destabilising for migraine-sensitive brains. When this clock receives irregular light inputs or is disrupted by stress or hormonal shifts, the timing of melatonin release can drift. This shift can influence sleep depth and the brain’s ability to stabilize sensory and pain-processing networks during sleep.
See also: why do migraines make you tired, blue light and migraines.
Insulin and Metabolic Hormones
Insulin helps regulate how the body uses and stores glucose, thus shaping the brain’s access to stable energy. When insulin levels fluctuate more quickly than usual or blood sugar rises and falls sharply, the brain may become more sensitive to internal or external migraine triggers. Shifts in insulin can also interact with metabolic hormones such as cortisol and estrogen, influencing how predictable energy and migraine patterns feel across the day.
Insulin helps maintain stable blood-sugar levels. Rapid shifts can lead to energy dips that may increase migraine sensitivity.
Skipped meals, long gaps between eating, or very carbohydrate-heavy meals can cause blood-sugar swings that increase vulnerability to symptoms.
Cortisol changes during stress can affect insulin function and blood-sugar stability in ways that influence hormonal migraine patterns.
People who are sensitive to reactive hypoglycemia, a rapid drop in blood sugar after eating, may notice migraines or aura symptoms after a sharp rise and fall in glucose levels.
Metabolic changes during life stages such as pregnancy or perimenopause, as well as times of sustained stress, can alter insulin responses and make migraine patterns feel less predictable.
Did you know?
The brain relies heavily on glucose for fuel, and insulin helps regulate how efficiently that glucose is delivered. When insulin signaling becomes irregular because of stress, disrupted eating patterns, or hormonal shifts, neurons may experience brief drops in energy availability, which can raise cortical excitability. Glucose delivery is sensitive to these changes, whereas alternative energy sources such as ketones enter the brain through transporters that do not require insulin. Since glucose delivery fluctuates with blood sugar levels, some people may be more prone to migraine symptoms when meals are delayed or blood sugar rises and falls quickly.
See also: migraine from low blood sugar, does sugar help migraines.
Thyroid Hormones
Thyroid hormones help regulate metabolic rate, energy availability, temperature balance, and overall physiological stability. When their levels rise or fall more than usual, the brain may find it harder to maintain steady energy and sensory processing, which can influence how readily migraine symptoms develop. Thyroid hormone fluctuations can also influence cortisol and estrogen, affecting how predictable migraine patterns feel across the day or month.
T3 and T4 help regulate how efficiently the body produces and uses energy. Changes in this balance can influence how steadily the brain functions.
Low thyroid levels may lead to fatigue, cold sensitivity, and slower energy metabolism, factors that can lower migraine thresholds.
High thyroid activity can raise heart rate, increase sensory alertness, and intensify heat sensitivity, which may heighten reactivity to triggers.
Thyroid shifts can modify cortisol and estrogen signaling, influencing downstream pathways involved in energy stability and sensory processing.
Pregnancy and postpartum changes, along with conditions that affect thyroid function, may influence how often migraines occur or how intense they feel.
Did you know?
Thyroid hormones help regulate mitochondrial activity, which in turn influences how efficiently neurons generate energy. When thyroid activity deviates from its normal range, mitochondrial output can become less stable, which may increase neuronal excitability. This increased excitability may raise migraine susceptibility during periods of altered thyroid activity, particularly when other hormonal or metabolic triggers are present.
See also: autoimmune and migraines.
Life Stages and Hormonal Patterns
Your hormone levels naturally shift as you move through life, and those changes can influence how predictable your migraine symptoms feel. Some life stages bring gradual hormonal transitions, while others involve quicker or more unpredictable shifts. During these periods, your brain may handle energy, sensory input, and migraine thresholds differently. Understanding how life stages shape hormonal patterns can make it easier to adjust your habits and manage symptoms as they change.
Puberty and Early Cycles
Puberty is often the first stage when hormonal changes start to shape how migraine symptoms develop. As estrogen and progesterone fluctuate more widely in early menstrual cycles, the brain’s energy and sensory systems can feel less stable, making it more reactive to changes in stress or daily demands. Since early cycles are often irregular, these shifting patterns can make migraine symptoms feel harder to anticipate. Some young people may notice that their migraine symptoms seem different from adult migraine, with more nausea, abdominal discomfort, or dizziness. This often settles as menstrual cycles become more regular.
During puberty, wide fluctuations in hormones can make migraine patterns harder to predict from month to month.
Early menstrual cycles are often irregular, with changes in timing or intensity affecting when migraines occur.
Some teens notice stronger sensory sensitivity, especially around light or sound, as hormonal patterns develop.
Aura may first appear during this stage, and many people find it becomes easier to recognize over time.
Growth-related changes, school stress, inconsistent sleep, and changing routines can amplify the effects of hormonal fluctuation.
Did you know?
The developing brain is particularly sensitive to changes in estrogen, which interacts with serotonin pathways that help regulate how sensory information is filtered and prioritized. When hormonal patterns are still settling, these pathways can feel less stable, which may help explain why migraine symptoms can first appear or shift during this stage of development. This temporary instability may lower sensory thresholds and increase cortical excitability, making migraine symptoms easier to trigger.
Menstrual Cycle
For many women, the menstrual cycle provides the clearest example of the link between hormones and migraine. As estrogen and progesterone rise and fall throughout the cycle, migraine sensitivity can shift in timing and intensity. Cycle-linked symptoms are often described informally as a hormonal migraine.
A sharp estrogen drop typically occurs before menstruation and can affect serotonin signaling, energy use, and sensory filtering.
Progesterone declines at the same time, which may increase neural reactivity in some people.
During the follicular phase, rising estrogen levels may support steadier energy and sensory processing, while ovulation-related fluctuations can increase sensitivity.
The luteal phase may feel stabilizing or challenging, depending on sleep quality, mood, and energy balance.
Menstrual cycle-related hormonal shifts may feel stronger when combined with poor sleep, stress, or irregular eating.
Did you know?
When estrogen levels fall before menstruation, serotonin availability can decrease, altering vascular tone and the reactivity of sensory pathways. This shift may increase cortical excitability, which can make neurons more likely to fire. When this happens alongside metabolic stress or poor sleep, the threshold for migraine activation can be lowered, which helps explain why migraines often cluster around the days just before a period begins.
See also: birth control for migraines.
Pregnancy and Postpartum
Pregnancy and the months after childbirth are periods of significant hormonal adjustment, and migraine patterns often change during this time. Some people notice an improvement in their symptoms during pregnancy, while others experience little change or new unfamiliar patterns. The postpartum period (the months after childbirth) can be a particularly sensitive time, as hormone levels shift rapidly, and sleep patterns and daily routines are often disrupted.
Over the course of pregnancy, estrogen and progesterone rise in a gradual manner, resulting in fewer abrupt hormonal shifts that affect migraine-related pathways. After delivery, both hormones drop quickly; this sudden change can influence energy regulation, sensory processing, and migraine thresholds.
During pregnancy, steadily rising estrogen levels may reduce rapid hormonal fluctuations that often influence migraine sensitivity.
Progesterone remains elevated throughout pregnancy, influencing sleep, calmness, and pain-modulating pathways.
Following childbirth, estrogen and progesterone levels fall rapidly, which can increase sensitivity in migraine-related pathways.
During the postpartum period, sleep disruption, physical recovery, and increased metabolic demand can interact with hormonal changes and affect migraine patterns.
Migraine patterns vary greatly during pregnancy and the postpartum period, often settling as hormone levels stabilize after delivery.
Did you know?
During pregnancy, the placenta produces hormones that help maintain steadier estrogen and progesterone levels. This added hormonal buffering reduces rapid fluctuations, which may help stabilize migraine-related brain pathways. After delivery, placental hormone production stops abruptly, contributing to the sudden hormonal withdrawal experienced in the postpartum period.
See also: migraine breastfeeding.
Perimenopause and Menopause
Migraine patterns often feel less predictable during perimenopause and menopause. This is because hormone levels do not decline in a smooth or predictable way. Instead of declining steadily, estrogen and progesterone can fluctuate widely before settling at lower levels. These hormonal shifts can influence energy regulation, sensory sensitivity, and day-to-day migraine thresholds.
Perimenopause, the transitional years leading up to menopause, is marked by irregular cycles and uneven hormone output, placing strain on systems involved in migraine regulation. Menopause begins once menstrual cycles stop, and while hormone levels are lower than during perimenopause, they tend to fluctuate less than during the transition phase.
During perimenopause, estrogen levels can rise and fall unpredictably, increasing sensitivity in migraine-related pathways.
Irregular ovulation during this stage can lead to inconsistent progesterone exposure, which may affect sleep, mood, and pain modulation.
Many women notice changes in migraine timing or intensity during perimenopause, even when their migraines were previously well controlled.
After menopause, estrogen levels are lower but more stable, and some women find their migraine patterns become more predictable over time.
Other factors such as sleep disruption, hot flashes, stress, and changes in energy regulation can interact with changing hormone levels and influence migraine sensitivity.
Did you know?
During perimenopause, large and unpredictable estrogen fluctuations can affect serotonin signaling, vascular tone, and neuronal excitability at the same time. When several migraine-related systems are stressed simultaneously, migraine thresholds can become less stable, which may make migraine timing feel harder to anticipate.
Hormone Replacement Therapy and Migraines
Hormone therapy, often referred to as hormone replacement therapy (HRT), is used to help manage menopausal symptoms by supplementing estrogen, sometimes alongside progesterone. If you have migraine, hormone therapy can influence symptoms in different ways, depending on the type of hormones used, how they are delivered, and individual sensitivity to hormonal change.
Because migraine is often sensitive to fluctuations in hormone levels rather than absolute levels, the goal of hormone therapy is usually stability rather than replacement alone. How hormones are introduced and maintained can matter as much as the dose itself.
Estrogen-containing hormone therapy can help some women by reducing hormonal swings, but may worsen symptoms if levels change too quickly.
Progesterone or progestogen can influence migraine patterns, especially in women sensitive to progesterone-related changes in mood, sleep, or pain modulation.
Transdermal delivery methods, such as patches or gels, tend to produce steadier hormone levels than oral hormone therapy.
For people with migraine, bioidentical hormone preparations are often preferred, particularly non-oral estrogen, as they tend to provide steadier levels of hormonal exposure than some synthetic or oral formulations.
Responses to hormone therapy vary widely, and what helps one woman may worsen symptoms for another.
Migraine responses to hormone therapy can differ depending on whether it is started during perimenopause or after menopause.
Some people with migraine report greater sensitivity to synthetic hormone formulations, particularly when these introduce hormonal instability or increase metabolic or oxidative strain.
Did you know?
For women with migraine, especially migraine with aura, stable estrogen levels usually matter more than the hormone level itself. Hormone therapies that provide steadier estrogen delivery may reduce abrupt fluctuations that can influence migraine thresholds, which is why the delivery method is often as important as the hormone type.
See also: hormone therapy for migraine sufferers.
Non-Hormonal Factors that Interact with Hormones
Hormones do not operate in isolation, with their influence on migraine being shaped by other biological and lifestyle factors. Even when hormone levels remain relatively stable, these factors can amplify or soften hormonal effects by influencing energy availability, stress responses, inflammation, and sensory processing.
Energy and metabolic factors
Skipped meals, irregular eating, or large swings in blood sugar can place additional strain on hormonal regulation, which may lower migraine thresholds.
Periods of increased energy demand, such as during illness, recovery, or sustained exertion, can affect hormonal balance and increase sensitivity.
Reduced mitochondrial efficiency or nutrient availability can make the brain less resilient to hormonal fluctuation.
Sleep and circadian rhythm
Poor or fragmented sleep can alter cortisol and melatonin rhythms that interact closely with estrogen and progesterone signaling.
Changes in sleep timing or light exposure can disrupt circadian rhythms and increase next-day sensitivity during hormonally active periods.
Chronic sleep disruption may make hormonal patterns feel more intense or unpredictable.
Stress and nervous system activation
Psychological or physical stress can increase cortisol and adrenaline levels and heighten sensory reactivity during hormonal transitions.
Ongoing physical or psychological stress may reduce the brain’s capacity to adapt to normal hormone fluctuations.
Coming out of a prolonged period of stress can trigger migraine in some people.
Inflammation and immune balance
Inflammatory activity can increase during times of hormonal change, particularly when the body is under stress or recovering from illness or injury.
Immune mediators, such as cytokines and histamine, may interact with estrogen signaling, influencing pain pathways and vascular responses.
Oxidative stress can further strain systems involved in hormonal and migraine regulation.
Environmental and lifestyle influences
Irregular routines, travel, temperature changes, or sensory overload can increase migraine sensitivity during hormonally active periods.
Alcohol, dehydration, or dietary triggers may have stronger effects during periods of hormonal fluctuation.
Physical tension in the neck and shoulders can contribute to overall migraine burden.
Taken together, these non-hormonal factors help explain why your migraine patterns can vary from month to month or even year to year, even when hormonal stages remain the same. You can support steadier energy, sleep, and stress regulation, which can reduce the overall load placed on hormone-sensitive systems.
See also:
Nutrition and metabolic support: Migraine nutrition, migraine micronutrient deficiencies, riboflavin, magnesium, and migraine, Magnesium and migraines, the riboflavin migraine mechanism, keto diet and migraines, medical foods.
Lifestyle and physical factors: migraines and drinking alcohol, heavy metals migraine, are migraines a neurological condition, teeth grinding and migraines, pillow for migraine sufferers.

Practical Strategies for More Stable Days
Making small, consistent adjustments to daily habits can help support steadier days and make migraine patterns feel more predictable over time.
Regular meals can help support steadier energy availability and reduce sudden drops in blood sugar.
Keeping sleep and wake times consistent can help support circadian stability.
Allow space for recovery during busy or demanding periods, particularly after illness, travel, or sustained stress.
Pacing your day and taking regular breaks can help prevent stress from building up.
Noticing early changes in sleep, appetite, or sensory sensitivity can help you adjust routines when possible.
These strategies are not meant to eliminate triggers or require perfect consistency.
Instead, they aim to lower the overall load on systems already sensitive to hormonal change, helping your body to adapt when fluctuations occur.
See also:
Diet and hydration support: what to eat if you have a migraine, foods that support migraine management, list of migraine foods to avoid, migraine elimination diets, breakfast ideas for migraine, electrolyte drinks for migraine.
Physical comfort strategies: physical therapy for migraine, heat, ice and migraine.
Brain Ritual® Support
Hormonal shifts can place extra strain on the systems involved in energy regulation, oxidative balance, sensory processing, metabolic regulation, and inflammatory signaling. During times when estrogen levels fluctuate or decline, particularly during hormonal transitions, the brain may become more vulnerable to oxidative stress and less efficient energy use, which can lower migraine thresholds.
Estrogen plays a protective role in the brain by supporting antioxidant balance and mitochondrial energy processes, while also influencing how the body regulates glucose and insulin. When estrogen levels fall or fluctuate, this protective effect can weaken, making the brain more sensitive to metabolic stressors and environmental triggers.
Brain Ritual® was developed to support these underlying brain systems through alternative fuel sources and targeted nutritional support. By supplying ketone-based energy alongside carefully selected micronutrients that support mitochondrial function and antioxidant balance, Brain Ritual® is designed to help stabilize energy availability and reduce metabolic strain during hormonally sensitive periods. You can learn more about the science behind Brain Ritual® here.
For some people, supporting steadier brain energy and oxidative balance may complement lifestyle strategies aimed at reducing the overall load on hormone-sensitive systems. This approach does not replace medical or hormonal treatments, but may offer additional support during times of increased vulnerability, such as perimenopause, postpartum recovery, or periods of sustained stress. If you’re interested in nutritional support designed for hormonally sensitive periods, you can find out more about Brain Ritual® here.
Disclaimer: Brain Ritual® is a medical food for the dietary management of migraine and is not intended to diagnose, treat, cure, or prevent any disease. This content is for informational and educational purposes only and is not intended as medical advice.
FAQs
What do people mean by “hormonal migraines”?
When people think of a hormonal migraine, they’re usually referring to hormonal migraine symptoms that seem to follow predictable hormonal patterns rather than a separate medical diagnosis. This often includes migraines that cluster around the menstrual cycle, pregnancy, postpartum recovery, or the perimenopause transition.
Hormonal migraine patterns reflect how changes in estrogen and progesterone influence brain energy regulation, sensory processing, inflammation, and migraine thresholds. For some people, symptoms feel more likely and can be more intense when hormone levels decline or fluctuate rapidly.
What causes migraines in females?
Migraines are more common in women because of natural hormonal fluctuations across the menstrual cycle, pregnancy, postpartum recovery, and perimenopause. During these times, changes in estrogen and progesterone can occur quickly or unpredictably.
These shifts can lower migraine thresholds by influencing brain energy availability, sensory processing, inflammation, and stress responses. Hormones do not cause migraine on their own, but when combined with factors such as stress, disrupted sleep, or irregular eating, they can make the brain more sensitive to triggers during hormonally active periods.
Is migraine in men related to hormonal change, or a different mechanism?
Migraine in men is not driven by the same large, cyclical hormonal fluctuations seen in women, but hormones still play a role. Men have more stable levels of sex hormones, particularly testosterone, which means they are less exposed to abrupt hormonal shifts that commonly lower migraine thresholds in women.
Hormones in men still influence many of the same systems involved in migraine, including energy regulation, stress responses, inflammation, and sensory processing. Changes in cortisol, adrenaline, insulin, and testosterone can all affect migraine susceptibility, especially during periods of stress, disrupted sleep, illness, or metabolic strain.
In this sense, the underlying migraine mechanisms are similar in men and women, but the pattern and magnitude of hormonal influence differ. In women, rapid estrogen fluctuations often act as a strong trigger. In men, migraine sensitivity is more likely shaped by interactions between stress hormones, metabolic factors, and nervous system regulation rather than by cyclical sex hormone changes.
Can hormones cause migraines?
Hormones do not directly cause migraine, but they can strongly influence how sensitive the brain is to triggers. Changes in hormones such as estrogen, progesterone, cortisol, and insulin can affect energy availability, neurotransmitter balance, inflammation, and sensory processing, all of which play a role in migraine susceptibility.
This is why migraine symptoms may appear or worsen during hormonal transitions, even when other lifestyle factors remain the same.
Are bioidentical hormones preferable for people with migraine?
Many clinicians suggest bioidentical hormone therapy for people with migraine, with a preference for non-oral estrogen delivered through patches or gels. This approach tends to produce steadier hormone levels. As migraine sensitivity is often driven by hormonal fluctuations rather than absolute levels, stability is usually the primary goal, particularly for systems involved in energy regulation and oxidative balance.
Bioidentical hormones are structurally identical to those produced by the body, and some people find them easier to tolerate than synthetic formulations. In contrast, certain synthetic or oral hormone preparations may introduce sharper hormonal shifts, which can increase sensitivity in migraine-related pathways. Responses vary, but prioritising formulation and delivery method is often an important consideration for migraine-sensitive individuals.
Hormones and migraines with aura: how are they linked?
Hormonal changes, especially rapid shifts in estrogen, can influence sensory pathways and cortical excitability in the brain. In people who already experience aura, these shifts may make visual or sensory symptoms more likely during certain phases of the menstrual cycle or during major hormonal life stages.
This may help explain why some people notice changes in aura frequency or intensity during menstruation, pregnancy, or perimenopause, and why symptoms such as blurred or altered vision can feel more prominent during hormonally sensitive periods.
What helps hormonal migraines feel more manageable?
Many people find that focusing on stability, rather than trying to eliminate every trigger, makes hormonal migraine patterns feel more manageable. Supporting steadier energy availability, consistent sleep patterns, and manageable stress levels may help reduce the overall load on systems sensitive to hormonal change, while paying attention to how symptoms shift over time can help clarify which strategies feel most useful.
How is estrogen withdrawal different from other hormonal fluctuations in migraine?
Estrogen withdrawal specifically refers to the sharp decline in estrogen before menstruation or after sustained high levels. Many studies show this drop is a key trigger in menstrual migraine, and is separate from steady or gradual changes in hormone levels.
Do hormones other than estrogen and progesterone play a role in migraine?
Yes. While estrogen and progesterone are the most studied hormones in migraine, other hormones and hormone-like signaling systems are also being explored. These include testosterone, oxytocin, and vasopressin, along with hormone-linked systems that shape neurotransmitter signaling related to pain processing, stress regulation, and neural excitability.
These systems may influence pain perception, stress responses, vascular regulation, and sensory processing. This in part helps explain why migraine also affects men, even though their hormone patterns tend to be steadier and are not tied to the menstrual cycle.
Research in this area is still developing, but it highlights that migraine sensitivity reflects a complex interaction between multiple hormonal and neurochemical systems, not estrogen and progesterone alone.
Can hormonal contraception, such as the contraceptive pill, affect migraine patterns?
Hormonal contraception can affect migraine patterns, particularly with formulations that contain synthetic estrogen or progestogens. Changes in hormone formulation or delivery method can influence brain energy regulation, sensory processing, and migraine thresholds, even when migraines were previously mild or infrequent.
Many people notice migraine symptoms emerging or changing weeks or months after starting the pill, rather than appearing immediately. This delayed response may reflect the cumulative effects of hormonal contraception on hormonal stability, oxidative stress, sleep, or metabolic balance, particularly in people who are already sensitive to metabolic or inflammatory strain. Responses vary, but worsening migraines or new aura symptoms can be a sign that a particular formulation is not well tolerated.
Why do hormonal migraine patterns change over time?
Hormone levels and rhythms naturally shift across different life stages, including puberty, pregnancy, postpartum recovery, perimenopause, and menopause. Each stage brings with it changes in how hormones fluctuate, how quickly they change, and how consistently they are produced.
As these patterns evolve, the brain’s energy use, sensory processing, and migraine thresholds can shift as well. This helps explain why migraine patterns may improve, worsen, or simply feel different as the body moves through these transitions.
Final Thoughts
Although hormones influence many systems involved in migraine sensitivity, they are only one part of the overall picture. Changes in estrogen, progesterone, stress hormones, and metabolic signaling influence how the brain handles energy, sensory input, inflammation, and recovery. When these systems become strained, migraine thresholds may feel lower and symptoms less predictable.
In reality, hormonal migraine patterns are rarely about a single hormone or one specific trigger. Rather, they reflect how multiple biological systems respond to change over time, through different life stages, and in response to everyday demands. This helps explain why migraine patterns may evolve, improve, or worsen even when hormone levels remain similar.
By focusing on stability and support, rather than control or elimination, it becomes easier to navigate hormonal migraine patterns more sustainably. An understanding of how hormones interact with energy, sleep, stress, and sensory processing can help you recognize vulnerable periods and adjust habits or support strategies accordingly, helping migraine patterns feel less random and more manageable over time.
See also: how to get rid of a migraine at home.
References
Beech, E. L., Riddell, N. J., & Murphy, M. J. (2023). Sex and stress hormone dysregulation as clinical manifestations of hypothalamic function in migraine disorder: a meta-analysis. European Journal of Neuroscience, 58(4), 3150–3171. doi:10.1111/ejn.16087. PMID: 37452646.
Del Moro, L., Rota, E., Pirovano, E., & Rainero, I. (2022). Migraine, Brain Glucose Metabolism and the “Neuroenergetic” Hypothesis: A Scoping Review. The Journal of Pain, 23(8), 1294–1317. doi:10.1016/j.jpain.2022.02.006. PMID: 35296423.
de Vries, T., et al. (2024). Sex differences in CGRP-induced vasodilation of human cerebrovascular tissues. Cephalalgia, 44(3), 201-214. doi:10.1177/03331024241254088.
Edvinsson, J. C. A., Grubor, I., Maddahi, A., & Edvinsson, L. (2024). Male-female comparison of vasomotor effects of circulating hormones in human intracranial arteries. The Journal of Headache and Pain, 25(1), 216. doi:10.1186/s10194-024-01933-w. PMID: 39663536.
Gonçalves, A. L., Martini Ferreira, A., Ribeiro, R. T., Zukerman, E., Cipolla-Neto, J., & Peres, M. F. P. (2016). Randomised clinical trial comparing melatonin 3 mg, amitriptyline 25 mg and placebo for migraine prevention. Journal of Neurology, Neurosurgery & Psychiatry, 87(10), 1127–1132. PMID: 27165014.
Islam, M. R., & Nyholt, D. R. (2022). Glucose-related traits and risk of migraine: A potential mechanism and treatment consideration. Genes, 13(5), 730. doi:10.3390/genes13050730. PMCID: PMC9141901; PMID: 35627115.
Nappi, R. E., Tiranini, L., Sacco, S., De Matteis, E., De Icco, R., & Tassorelli, C. (2022). Role of Estrogens in Menstrual Migraine. Cells, 11(8), 1355. https://doi.org/10.3390/cells11081355
Raffaelli, B., Neeb, L., & Reuter, U. (2023). Menstrual migraine is caused by estrogen withdrawal: Revisiting the evidence. Journal of Headache and Pain, 24(1), 68. PMID: 37184042.
Seidkhani-Nahal, A., Esfahani, M. M., & Togha, M. (2021). Thyroid hormone levels in migraine: A systematic review and meta-analysis. Hormones, 20(2), 139–149. doi:10.1007/s42000-020-00228-4. PMID: 32666358.
Stubberud, A., Buse, D. C., Kristoffersen, E. S., Linde, M., & Tronvik, E. (2021). Is there a causal relationship between stress and migraine? Current evidence and implications for management. The Journal of Headache and Pain, 22, 155. doi:10.1186/s10194-021-01369-6.
Tasnim, S., Wilson, S. G., Walsh, J. P., Nyholt, D. R., & International Headache Genetics Consortium (2023). Shared genetics and causal relationships between migraine and thyroid function traits. Cephalalgia, 43(2), 333–10242221139253. doi:10.1177/03331024221139253. PMID: 36739509.
van Lohuizen, R., Paungarttner, J., Lampl, C., MaassenVanDenBrink, A., & Al-Hassany, L. (2024). Considerations for hormonal therapy in migraine patients: a critical review of current practice. Expert Review of Neurotherapeutics, 24(1), 55–75. https://doi.org/10.1080/14737175.2023.2296610
Vetvik, K. G., & MacGregor, E. A. (2021). Menstrual migraine: a distinct disorder needing greater recognition. The Lancet Neurology, 20(4), 304–315. doi:10.1016/S1474-4422(20)30482-8. PMID: 33600767
Waliszewska-Prosół, M., Grandi, G., Ornello, R., Raffaelli, B., Straburzyński, M., Tana, C., & Martelletti, P. (2025). Menopause, perimenopause, and migraine: Understanding the intersections and implications for treatment. Neurology and Therapy, 14(3), 665–680. doi: 10.1007/s40120-025-00720-2. PMCID: PMC12089631; PMID: 40085393.